Save the Planet, Kill Your Patient
The dark implications of an increased focus on social and environmental "justice" in medicine

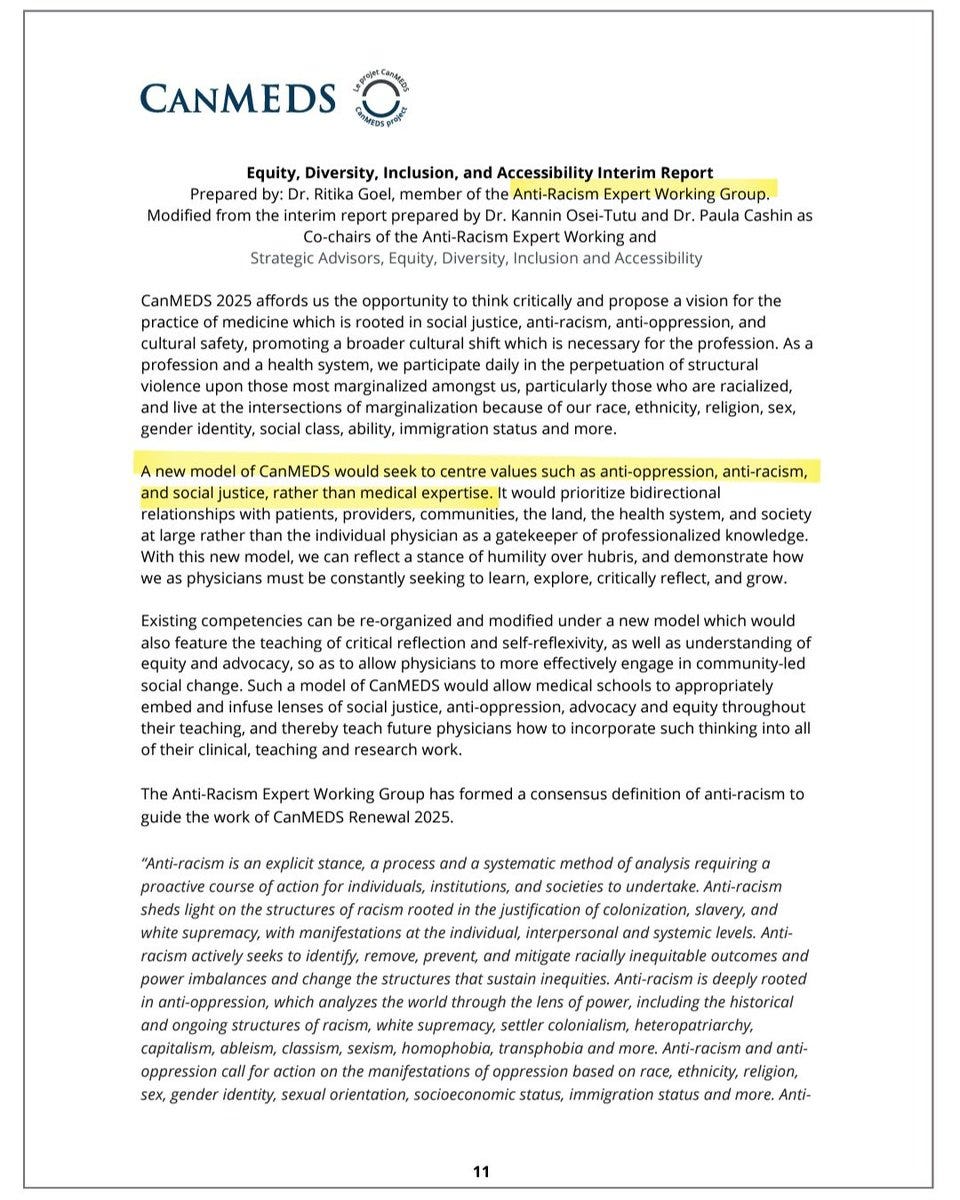
Last week, a subcommittee of the Royal College of Physicians and Surgeons of Canada (the organization which oversees and grants credentials to medical specialists in this country) produced a report recommending changes to its “CanMEDS” educational framework. The Royal College defines CanMEDS as “a framework that identifies and describes the abilities physicians require to effectively meet the health care needs of the people they serve.”

You might think these abilities would include things like mastering diagnostic criteria and safe prescribing practices, or demonstrating the technical skills appropriate to one’s area of medical expertise. But if this committee gets its way, CanMEDS will no longer focus on medical expertise as the primary goal of specialist medical education. Rather, the “new model of CanMEDS would seek to centre values such as anti-oppression, anti-racism and social justice.”
This report is remarkable not because of its ideologically extreme position—at this point almost every medical organization has been captured by the far left—but because they actually said the quiet part out loud: social justice rather than medical expertise.
The most obvious implication of this plan would be a new generation of physicians and surgeons who are less competent and more “woke” than their predecessors, which is terrifying enough in and of itself: If I’m about to have my gallbladder removed, I want my surgeon to be excellent at removing gallbladders and I don’t care one iota whether he or she can quote Robin DiAngelo and Ibram X. Kendi. And let’s face it, there are only so many hours in a week. Every hour a medical resident spends learning about “anti-racism” and “analyzing the world through the lens of power” is one hour not spent practicing gallbladder surgery.
This degradation of the quality of medical education goes hand in hand with the lowering of standards for medical school admission and hiring—already well underway—as more and more schools move away from strictly merit-based standards and toward ideological purity tests (applicants at many schools are required to submit pledges to promote diversity, equity and inclusion) and the preferential admission of certain preferred identity groups:

The Royal College is not alone, of course. South of the border, The American Medical Association has already adopted a plan to “embed racial justice and advance health equity” in “the healthcare system and other social institutions.” And it seems like you can’t pick up a medical journal these days without half the articles looking like they’d be more appropriate in the sociology or environmental studies section. Save the planet! Be an anti-racist! Respect the pronouns of pregnant people! And did I mention health equity?
Calls for “health equity” are everywhere. (Coincidentally, the ad for the Harvard online course pictured below arrived in my inbox as I was working on this Substack.) To the uniformed—who are still under the mistaken impression that “equity” is the same thing as “equal treatment”—this sounds like a benign enough idea.

In reality, equity (and its sister terms like “anti-racism”) often mean quite the opposite of equal treatment. In healthcare, it means ensuring equal health outcomes between groups (especially racial groups) by whatever means necessary, even if that requires treating one group preferentially. Hippocratic Oath be damned. As James Lindsay recently put it, we have thrown out the concept of “Do No Harm” in favour of “redistributing harm.”

If you think this doesn’t yet have real world implications, think again. At the peak of the COVID pandemic, when treatments such as monoclonal antibodies and anti-viral medications were being rationed, New York and other states prioritized non-white individuals for treatment. Canada followed a similar strategy in prioritizing vaccines (remember, those vaccines SO critical for your health that it was mandatory to get them?) for indigenous citizens. Young, healthy people were vaccinated ahead of 90-year-old diabetics with bad lungs, as long as those young people were part of a preferred racial group.
As FSIM alumnus Dr. Aaron Kheriaty has pointed out, when doctors switch their focus from the well-being of their individual patient to the promotion of some larger societal goal, bad things inevitably ensue. EVIL things. The most glaring example of this is what happened to medicine in Germany—considered among the best in the world at the time—in the 1930’s:
In 1922, Alfred Hoche and Karl Binding, a psychiatrist and a lawyer, published an influential book, Allowing the Destruction of Life Unworthy of Life. A metaphor from this and other influential works captured the imagination of the German medical establishment, undermining the traditional Hippocratic ethic that had governed medicine since antiquity.
Instead of serving the health of the individual patient presenting for treatment, German physicians were encouraged to be responsible for the “health” of the “social organism”—the volk—as a whole.
Instead of seeing afflicted individuals as sick and in need of compassionate medical care, German doctors became agents of a socio-political program driven by a cold and calculating utilitarian ethos. If the social organism was construed as healthy or sick, some individuals (e.g., those with cognitive or physical disabilities) were characterized as “cancers” on the volk. And what do doctors do with cancers but eliminate them?
The first people gassed by the Nazis were not Jews in concentration camps (that came later), but disabled patients in psychiatric hospitals, murdered under the Third Reich’s “T4 Euthanasia Program.” Each of these death warrants was signed by a German physician. Even after the lethal regime turned its attention on Jews and other ethnic minorities, they continued to deploy quasi-public health justifications: Recall that the Jews were routinely demonized by the Nazis as “spreaders of disease.” If physicians serve not the needs of sick and vulnerable patients, but are agents of a social program, the German example shows us what happens when that social program is misdirected by a corrupt regime.
Forgive me, then, for finding it a tad creepy when physician environmentalists at the recent UN climate change meeting performed CPR on an inflatable model of the earth and described the planet as “running a fever.” Or when “anti-racist” guru Ibram X. Kendi proclaimed that “this nation has metastatic racism….and in order for us as a country to be healed, there's going to be pain, and there's going to be a tremendous amount of pain.”
What is the logical conclusion of this type of language? Of this type of thinking? Whence leads this potentially slippery and dangerous slope? If a physician thinks that “racial justice” or “the climate emergency” are existential threats, then everything and anything can be justified pursuing and promoting them.
If I, as a physician, truly believe that my primary job is to promote racial "equity" (equality of outcome between racial groups) and to help reduce CO2 emissions, how will I treat, say, an elderly white patient with dementia or advanced heart failure? The logical answer would be to “euthanize” them. That, I fear, is where we are headed if we don't fight back against this insanity.
—Julie
Thank you very much for yet another outstanding article highlighting the pervasive influence of Woke far-left culture, which has surreptitiously infiltrated our once-thought-to-be free society. Canada, like many Western countries, is now witnessing the stifling of voices, leading to people being "cancelled" and losing their jobs and livelihoods.
I was heartened to observe a strong opposition to the Royal College's proposal to alter CanMED by numerous readers of The Medical Post just a few days ago. It seems that people are growing weary of the encroachment of this problematic woke culture, intent on undermining the foundations of a free world.
On a tangential note, I must mention that today, another piece with a woke-style perspective was published in the Medical Post, focusing on "weight-equitable" care. The article suggests that discussing the impact of obesity on health with patients is detrimental to their self-esteem and should be avoided. Initially, I thought it was a jest as I started reading, only to realize, regrettably, that it was not.
Once again, thank you for shedding light on these pressing issues and for providing a platform to discuss the challenges posed by the pervasive influence of woke ideologies.
Great piece. Why I support you guys. This is going to be a fight that lasts all our lives. Worse, the woke social justice warriors curre tly ignoring mass rape and murder in Israel because of their own anti Semitism - taught to them by those higher education social justice elements/groups/individuals like Claudine Gay who make a great living and exercise major personal power by wielding the threat of them coming after wrong think (starting with speaking up in the first to refute the ways social justice goes wrong in practice) - those students graduating today haven't yet begun to truly spread into positions of power in govt. On an individual level this is a massive risk to you me our living standards and our freedom.
But it gets worse.
Our strategic enemies love and invest billions every year promoting this discord and division. They love the weakening of the commitment to freedom that is the heart of democratic systems. And it's not the social justice people who defend it. They would rather tear the system that built our free way of life down.